by MITA MISTRY
I recently read a study in the British Medical Journal on the barriers to accessing mental health services in the BAME community and felt compelled to write this.
People from ethnic minorities are less likely to contact their GP about mental health, take antidepressants or receive specialist care than their white British counterparts. And the prevalence of anxiety and depression in south Asian women is higher than white women (63.5 per cent compared with 28.5 per cent). Sadly, the BAME community are more likely to have poorer health outcomes and shorter life expectancy.
It’s unclear whether the disparities in access to mental health services reflect the diverse BAME mental health needs or are the result of institutional, cultural or socioeconomic exclusion factors.
According to this study, there are some key barriers to accessing mental health services. For example, some people feel uncomfortable talking to doctors or healthcare professionals because they do not ‘get’ their cultural needs. There is also an issue where language is concerned as it can be hard to articulate feelings and thoughts when English is not your first language. Equally, it’s harder for doctors to make a diagnosis.
Many people are unaware of the services available or how to access them, so rely on the community and social networks in times of a crisis. But if these social networks don’t exist, say for recent immigrants or those living alone, there is a feeling of sheer isolation.
Sometimes the community acts as an alternative to professional help, which is not always enough for people. Recently, a mother told me that her bereaved son had not cried at all since the passing of his wife and was struggling to process his grief. I asked if they had considered counselling to which she replied, “no, he will be fine, we don’t need that.”
It shows a cultural stigma towards mental health is still a problem within Asian communities where the expectation is to be strong and deal with what life throws at you.
And some fear a mental health diagnosis could stigmatise the entire family or see it as a failure, thus affecting their respect in the community. But the problem with stigma towards mental health and ‘culturally unacceptable’ behaviours associated with common problems like anxiety, depression and addictions mean people are reluctant to openly address their symptoms and get the help they truly need.
So what can we do about it? First, the importance of tackling these barriers is paramount. And the good news is The National Service Framework for Mental Health has plans for healthcare providers to deliver culturally sensitive care. But as a community, we need to accelerate shifting attitudes towards mental health and take it more seriously. Opening up is a start, but we also need to be informed of the conditions, symptoms, personal wellbeing and services that can help.
There is no shame in seeking professional help if you are struggling with your emotions and thoughts. Mental health issues do not make you weak; they mean you are human. Nobody should be made to feel alone or suffer in silence and every single person deserves to heal.
www.mitamistry.co.uk & www.twitter.com/MitaMistry



 Fitbit users begin automatic transition into Google Health app experienceGoogle Health
Fitbit users begin automatic transition into Google Health app experienceGoogle Health  Personal health data from multiple sources appears in one dashboardGoogle Health
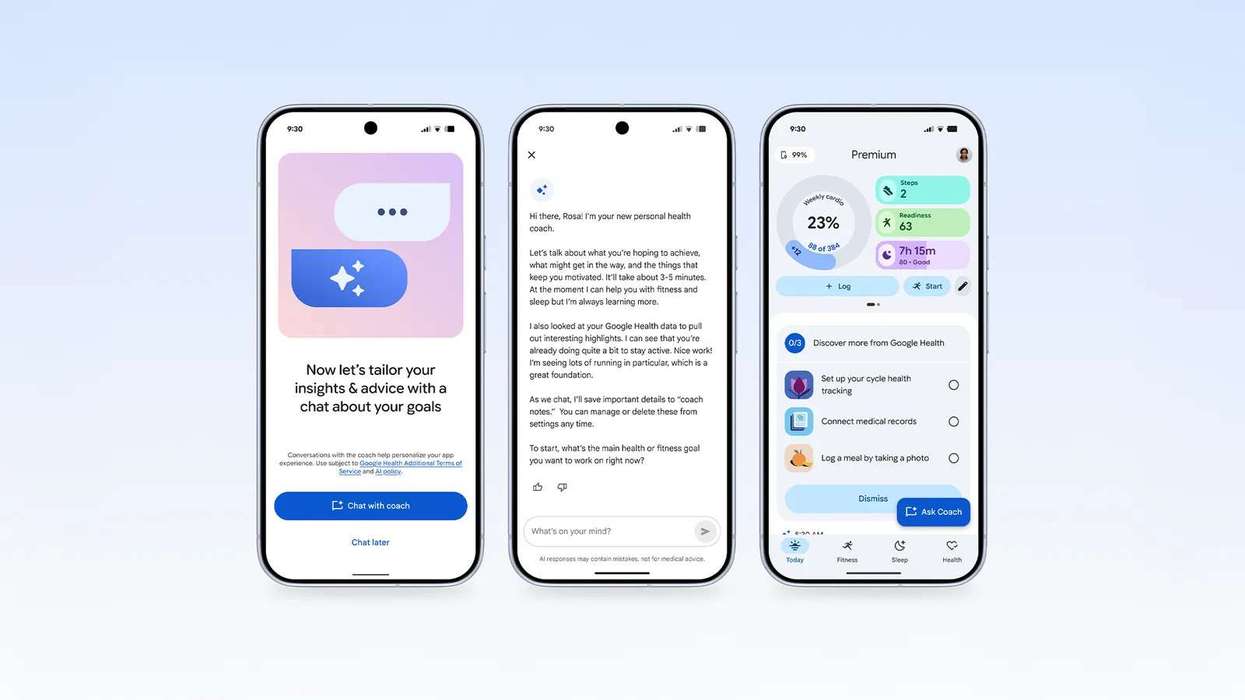
Personal health data from multiple sources appears in one dashboardGoogle Health 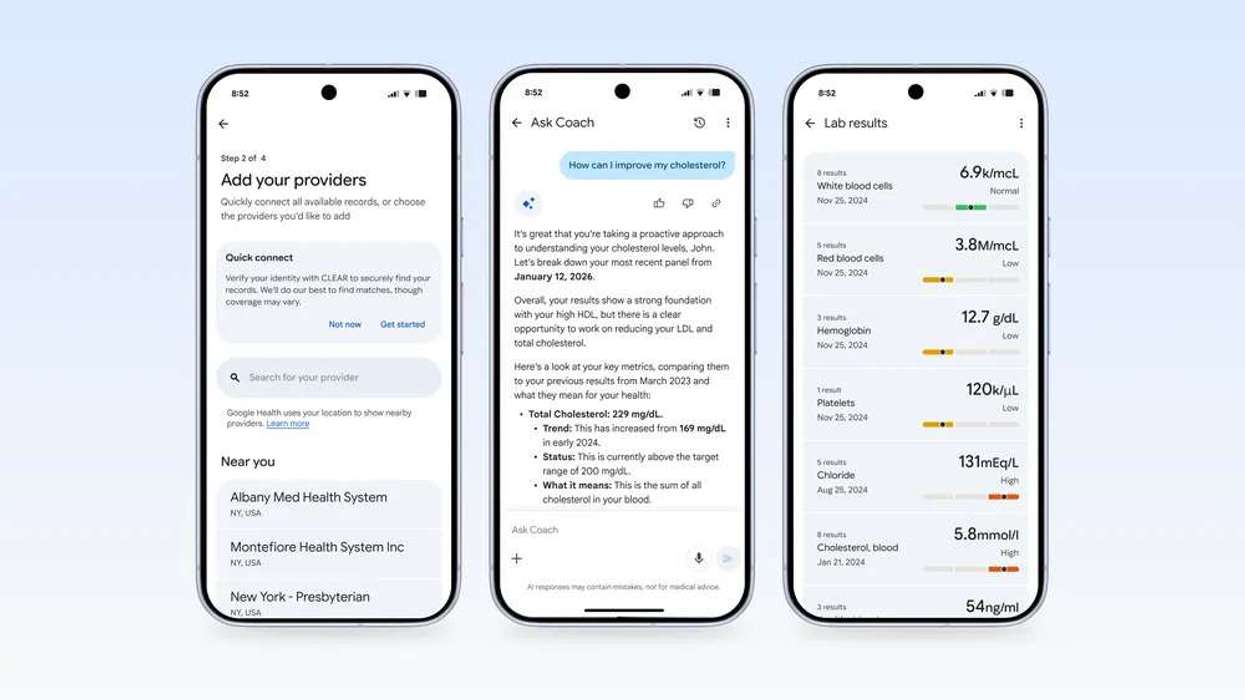 AI Health Coach offering personalised guidance for daily wellness routinesGoogle Health
AI Health Coach offering personalised guidance for daily wellness routinesGoogle Health 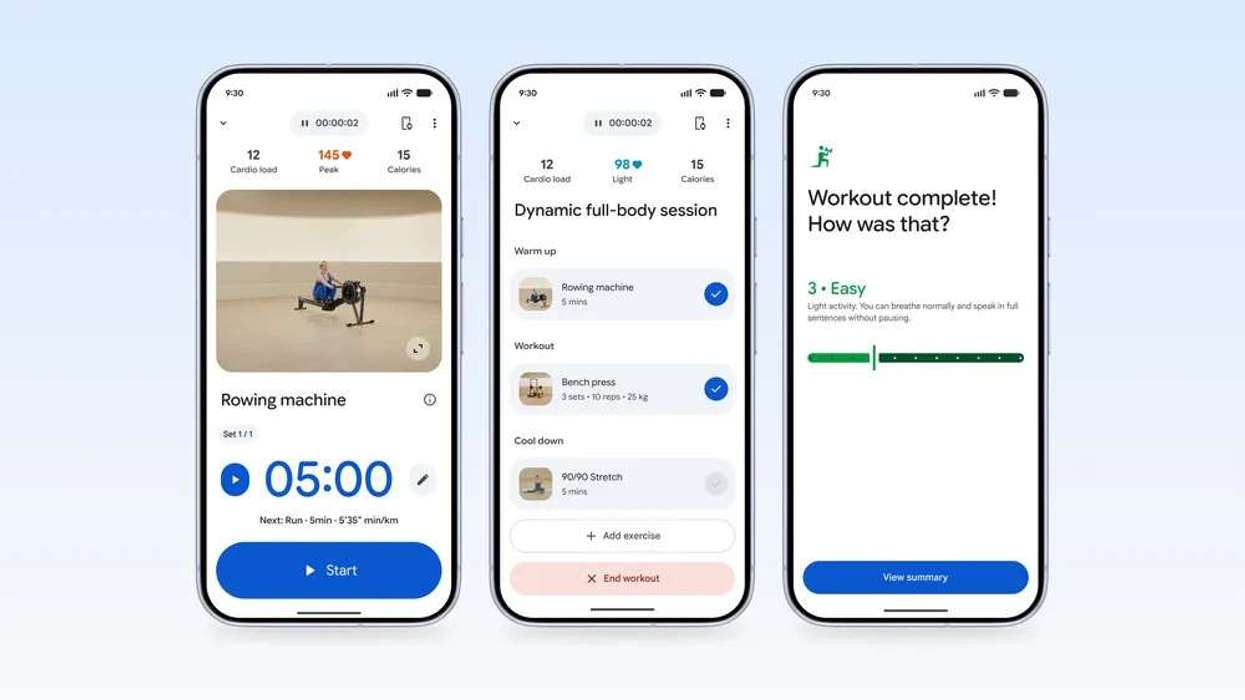 Health data can be securely shared with doctors and family membersGoogle Health
Health data can be securely shared with doctors and family membersGoogle Health 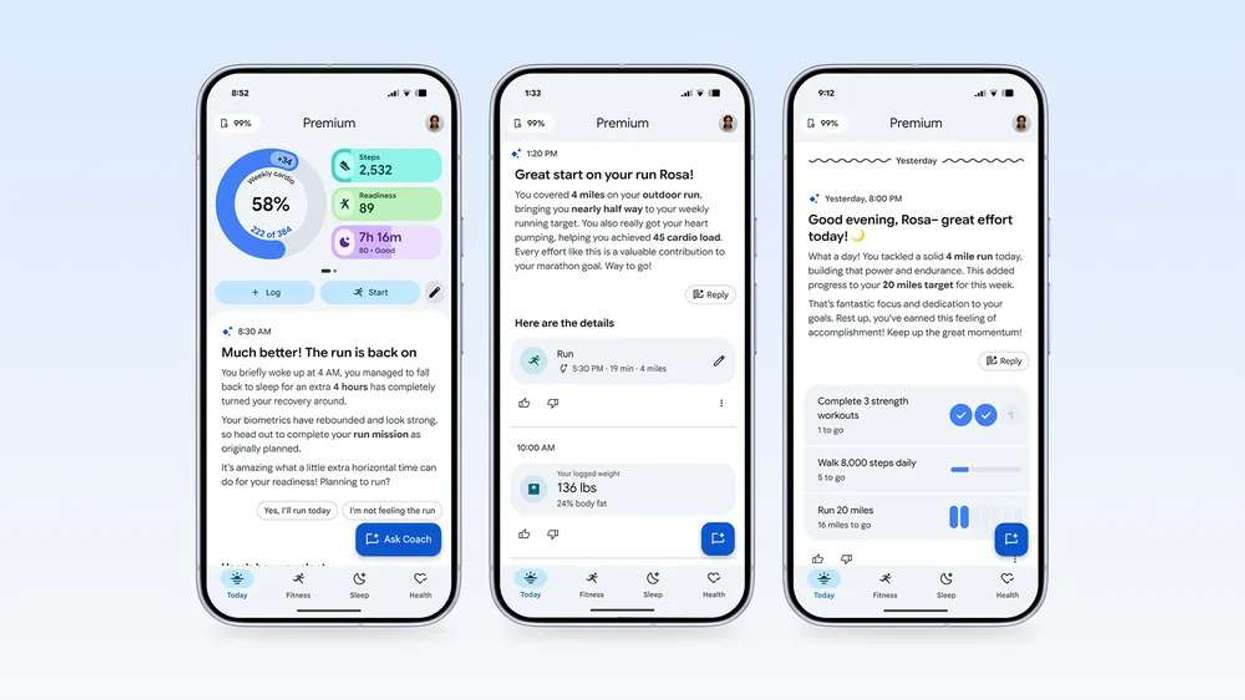 Advanced AI features unlocked through optional Google Health Premium subscriptionGoogle Health
Advanced AI features unlocked through optional Google Health Premium subscriptionGoogle Health